先說在前面,繩梯式打法(Rope Ladder)還是目前的主流,扣眼式打法只建議用在一部分的病人上面,原因是…
Randomized controlled trial (RCT)
觀察性研究(observational study)或是世代性性研究(cohort study)我就不整理了,我就直接列證據等級最高的RCT(隨機對照試驗)五個,並且把他和我們臨床上面最關心的問題(出血、感染、…等)結果來列表。(CJASN在2019三月有一篇加拿大的RCT做在居家透析病人上面,不過n=14....我想應該沒有放進來的價值)
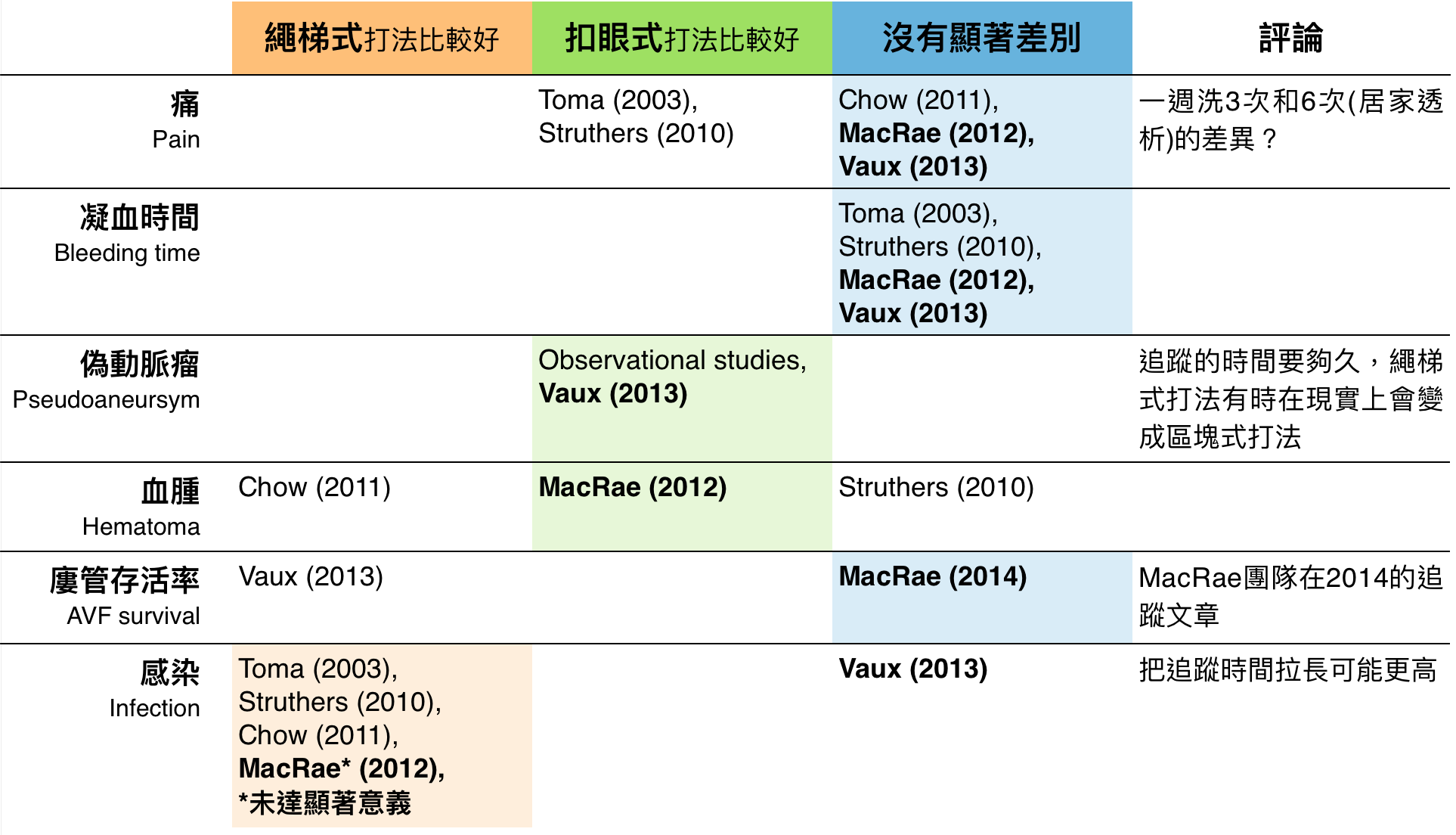
我們可以很持平誠實的說,大多數我們預期的好處,像是凝血問題、疼痛、樓管存活率等等,並沒有在嚴謹的試驗中看到信服的證據。
唯一比較有明顯勝出的是固定位打法可以顯著減少偽動脈瘤的產生,推測原因是繩梯式打法有時候受限於現實的條件,有時候和區塊式打法有八成像XD
而很要命的是,近乎所有的臨床試驗都顯示了固定位打法有較高的感染機會。
唯一不合群的是2013的Vaux et al.,但這個試驗有幾個特點我想特別拿出來講講
Nephology, Dialysis, Transplantation(腎臟科很熟悉的NDT)在2016年有針對固定位打法做過專題討論(免費公眾閱覽 [open access] 由此去. Volume 31, Issue 4, April 2016)。進行總結的Moderator Laura Labriola(比利時)對Vaux et al.感染率的結果,認為和上述三點可能都有關聯。
該篇專題討論也花了不少篇幅在討論未來可以改善感染率的作法(見連結表格),不過在感染的疑慮真的解決之前,主流意見多半認為固定位打法不適合全面性無差別的使用。
都適合的情況下,方能為病患提供最大的福祉。
2006 KDOQI 2006 Vascular access update
有自體動靜脈廔管的病人應該把扣眼式打法納入考慮
2007 European Vascular Access Society
繩梯式打法是首選,而自體動靜脈廔管的病人,尤其是可以上針的範圍很局限的病人,扣眼式打法比區塊式打法好
2015 United Kingdom Renal Association
自體動靜脈廔管的病人推薦使用繩梯式打法和扣眼式打法,人工血管的病人應該使用繩梯式打法
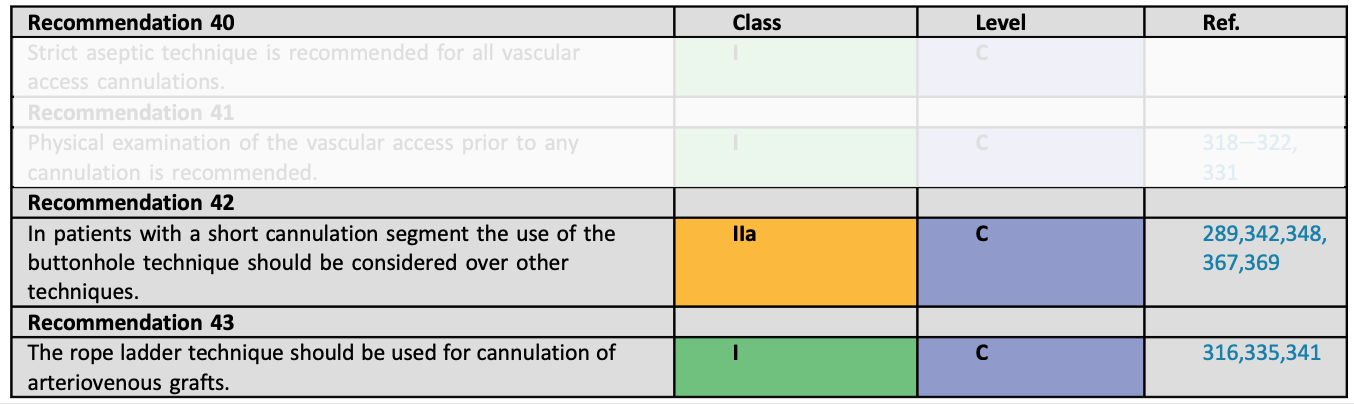
2018 Clinical Practice Guidelines of the European Society Vascular Surgery (ESVS)
目前文獻不支持常規性的在所有自體動靜脈廔管的病人使用扣眼式打法,不過此法可能特別適合廔管過短的病人
扣眼式打法(Buttonhole technique)之二:Constant site method的發明者:Twardowski醫師
扣眼式打法(Buttonhole technique)之三:投一次沒人看,你有投兩次嗎?
扣眼式打法(Buttonhole technique)之四:目前實證研究證據以及Guideline整理
Randomized controlled trial (RCT)
隨機對照試驗整理
觀察性研究(observational study)或是世代性性研究(cohort study)我就不整理了,我就直接列證據等級最高的RCT(隨機對照試驗)五個,並且把他和我們臨床上面最關心的問題(出血、感染、…等)結果來列表。(CJASN在2019三月有一篇加拿大的RCT做在居家透析病人上面,不過n=14....我想應該沒有放進來的價值)
我們可以很持平誠實的說,大多數我們預期的好處,像是凝血問題、疼痛、樓管存活率等等,並沒有在嚴謹的試驗中看到信服的證據。
唯一比較有明顯勝出的是固定位打法可以顯著減少偽動脈瘤的產生,推測原因是繩梯式打法有時候受限於現實的條件,有時候和區塊式打法有八成像XD
而很要命的是,近乎所有的臨床試驗都顯示了固定位打法有較高的感染機會。
唯一不合群的是2013的Vaux et al.,但這個試驗有幾個特點我想特別拿出來講講
- 使用Nipro的Biohole設備,特色是在建立通道的初期(至少六次),用一個polycarbonate peg聚碳酸脂的栓子(Biohole plug),在透析後拔針之後,插入並留置在針進出的那個通道,使通道更穩固。
- 追蹤的時間是一年。(追蹤時間最長的是MacRae et al.,平均一年半)
- 試驗期間,Buttonhole扣眼式打法的組別有高達三分之一dropout,改成Rope ladder繩梯式打法
Nephology, Dialysis, Transplantation(腎臟科很熟悉的NDT)在2016年有針對固定位打法做過專題討論(免費公眾閱覽 [open access] 由此去. Volume 31, Issue 4, April 2016)。進行總結的Moderator Laura Labriola(比利時)對Vaux et al.感染率的結果,認為和上述三點可能都有關聯。
該篇專題討論也花了不少篇幅在討論未來可以改善感染率的作法(見連結表格),不過在感染的疑慮真的解決之前,主流意見多半認為固定位打法不適合全面性無差別的使用。
除了因為動靜脈廔管過短造成無法使用繩梯式打法的病人外,應該在
- 天時(自體動靜脈廔管的病人,有設計良好的器材e.g.像是polycarbonate peg聚碳酸脂的栓子 )
- 地利(不要太繁忙、每次打針都不同護理人員、或是人員流動大的透析中心)
- 人和(能夠嚴謹地每一次都遵守打針、感染控制SOP的病人)
都適合的情況下,方能為病患提供最大的福祉。
Guideline臨床準則怎麼說?
以下節錄從古至今有提到扣眼式打法的臨床準則(Guideline)2006 KDOQI 2006 Vascular access update
有自體動靜脈廔管的病人應該把扣眼式打法納入考慮
3.3 Buttonhole:
Patients with fistula access should be considered for buttonhole (constant-site) cannulation. (See protocol in CPG 3.)
2007 European Vascular Access Society
繩梯式打法是首選,而自體動靜脈廔管的病人,尤其是可以上針的範圍很局限的病人,扣眼式打法比區塊式打法好
Guideline 4.4. The rope ladder technique should be used for cannulation of grafts (Evidence level III)
In autogenous fistulae, particularly those with only a short vein segment available for needling, the buttonhole method is preferred over area puncture.
2015 United Kingdom Renal Association
自體動靜脈廔管的病人推薦使用繩梯式打法和扣眼式打法,人工血管的病人應該使用繩梯式打法
6. Maintenance of vascular access (Guidelines 6.1-6.5)
Guideline 6.1 – Needling technique
We recommend that the rope-ladder and buttonhole techniques should be used for cannulation of AVF and rope-ladder for AVG (2B).
2018 Clinical Practice Guidelines of the European Society Vascular Surgery (ESVS)
目前文獻不支持常規性的在所有自體動靜脈廔管的病人使用扣眼式打法,不過此法可能特別適合廔管過短的病人
6.3.2.5. Buttonhole technique
Currently, the available literature does not recommend the routine use of the buttonhole method in all AVFs. However, the buttonhole cannulation technique may be especially appropriate for patients with a short cannulation segment
條目
扣眼式打法(Buttonhole technique)之一:簡介扣眼式打法(Buttonhole technique)之二:Constant site method的發明者:Twardowski醫師
扣眼式打法(Buttonhole technique)之三:投一次沒人看,你有投兩次嗎?
扣眼式打法(Buttonhole technique)之四:目前實證研究證據以及Guideline整理
參考資料
- Labriola L et al. Moderator’s View: Buttonhole cannulation of arteriovenous fistulae: Great caution is warranted. NDT. 2016; 31: 530–533.
- Toma S et al. A timesaving method to create a fixed puncture route for the buttonhole technique. NDT. 2003; 18: 2118–2121.
- Struthers J et al. Buttonhole Needling of Ateriovenous Fistulae: A Randomized Controlled Trial. ASAIO J. 2010; 56: 1
- Chow J et al. A randomised controlled trial of buttonhole cannulation for the prevention of fistula access complications. J. Ren. Care 2011; 37: 85–93.
- MacRae JM et al. A randomized trial comparing buttonhole with rope ladder needling in conventional hemodialysis patients. CJASN. 2012; 7: 1632–1638.
- Vaux E et al. Effect of buttonhole cannulation with a polycarbonate peg on in-center hemodialysis fistula outcomes: A randomized controlled trial. AJKD. 2013; 62: 81–88.
- MacRae JM et al. Arteriovenous fistula survival and needling technique: Long-term results from a randomized buttonhole trial. AJKD. 2014; 63: 636–642.
Next
« Prev Post
« Prev Post
Previous
Next Post »
Next Post »